Trust and transparency: GP Data for planning and research
Wednesday, 16 June, 11.00 - 12.30
In this webinar, we explored the circumstances around the proposed GP Data for Planning and Research (GPDPR). In particular, we wanted to give patients, relatives and carers the opportunity to communicate directly with those in charge of the programme, and with a wider panel with different perspectives. We wanted a dialogue about the GDPDR, to ensure there is a balanced debate about anticipated benefits versus potential risks. The webinar was devised by patients to bring a patient voice to the discussions.
We heard about the development of the GPDPR, its aims and ambitions. We then explored with delegates what needs to be done to make the GPDPR a success, in the interests of patients.
The webinar panel
Phil Booth, Coordinator, MedConfidential
Dr Nicola Byrne, National Data Guardian
Dr Arjun Dhillon, Caldicott Guardian, NHS Digital
Prof Mark Lawler, Scientific Director for DATA-CAN, the HDR-UK Hub for Cancer
John Marsh, Advisory Group Member, use MY data
Dr Geoff Schrecker, Retired GP, Retired chair of EMIS National User Group, Deputy Chair IGARD, RCGP Clinical Champion for Patient Data Choices
The panel chair was Chris Carrigan, Expert Data Adviser to use MY data. The initial introduction to the GPDPR was given by Dave Roberts, Head of Primary Care Information at NHS Digital.
The webinar can be watched by clicking the video box to the right and the introduction slides are available below. The panellists did not use slides. During the course of the 90 minute webinar, the delegates raised nearly 120 questions, clearly highlighting the need for much wider consultation and information about the GPDPR.
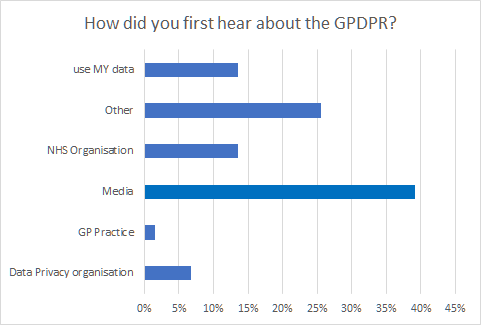
At the start of the webinar, we asked delegates to respond to some initial poll questions. Our first question was to help understand how delegates had first heard about the GPDPR. The results are shown below:
By far the largest source of information available to delegates about the GPDPR had been from the media
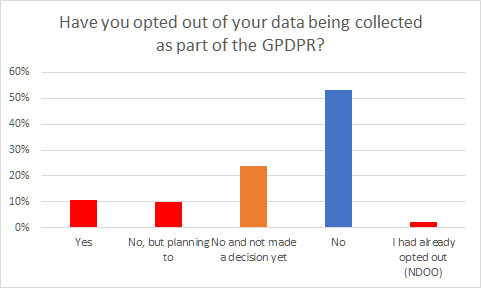
To understand the effects of the publicity about the GPDPR, we asked our delegates whether they had yet decided whether to opt out or not. Clearly with this being a use MY data event, there could be an expectation that delegates could lean towards the 'using data' end of the spectrum, but the results that we found are shown below:
The GPDPR publicity has already had a significant effect on behaviour - over 20% of delegates have either already opted out in some capacity already, or are intending to
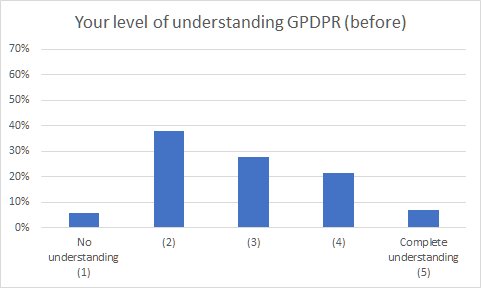
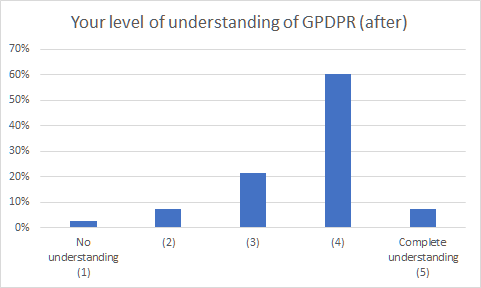
We ran a poll at the start of the webinar to gauge delegates’ level of understanding about the GPDPR and we repeated the poll at the end of the webinar. The results are shown below:
The level of understanding of the GPDPR amongst most delegates increased significantly as a result of the webinar
Key themes raised during the webinar
A set of key themes, issues and actions were raised by and with our Panel Members, which are shown below. We would also encourage you to watch the full webinar recording.
Theme: The mechanism of opt out is unclear to people and difficult in the current situation - we have seen over 100,000 new National Data Opt-outs in a month, despite these not being the route required to express a GPDPR opt out. We do not know the number of Type-1 opt outs made via GP practices.
To opt-out of your data being used as part of GPDPR, you need to record a 'Type-1' opt out with your GP Practice
No information is available about the numbers of 'Type-1' opt-outs, or the effect of the recent publicity around GPDPR
But there have been an additional 100,000 National Data Opt-outs in May 2021 alone
We have not yet heard a clear explanation what data will leave our GP practice, and what data will stay. “Need to make it absolutely clear to the public that they have two opt-out choices”
"Why hasn’t NHS Digital made clear the differences between the two opt outs and WHY has NHS Digital made the Type 1 opt out for the GPDPR simple and clear to opt out. That was a CHOICE and not an accident"
This is confusing, and the feedback from the last few weeks makes this clear
Should the National Data Opt-out be a singular statement and line?
"I am concerned that patient opt-out is lip service and in shambles, from what I hear so far which only fuels my hesitancy"
"It sounds like we can opt out but we don't know what we are opting out of. And even if we do the system does not ensure that the opt out(s) are adhered to. I don't believe they really have the systems to manage this in a way that patients have a right to expect"
use MY data believes that patients can only make an informed decision when clear, complete and comprehensible information is available to them, in an accessible form, incuding information about how to opt out and what this means. If patients object to the sharing of their data, these objections should be respected.
Theme: The timing of the proposed 'go-live' date is too short. Effective communication with patients and the public is needed, so that they have enough time to make an informed choice. Our delegates posted nearly 120 questions during the webinar, most of which we did not have time to answer.
"The decision needs to be delayed to give the public a chance to engage, just giving them August when its a holiday month makes no sense"
Language around 'grabbing / scraping data' are concepts close to the idea of exploitation
We heard plans about public communication from NHS Digital: 'We will soon launch a substantial campaign to publicise this activity and tell people about their choices which will run throughout the summer'
People’s concerns about commercial interests have been prominent. The National Data Guardian's office has done work on assessment of public benefits
There must be a continued emphasis on the importance of transparency & 'authentic public engagement'. Highlighting that public benefit must outweigh commercial interest, at all times
"Public and patient voices are essential to weave into this if trust is to be rebuilt - but listening takes time and time is very short if 1 Sept deadline is to stand"
"The ability to use data to improve people's health is a worthy target, so I need you to make sure the thing is secure and clearly explained so I can then go to the various patient council bodies I am on and give a nice clear explanation to our members"
use MY data agrees with the decision taken by NHS Digital to delay the implementation of the GPDPR. But the September 2021 deadline is too short to ensure patients have enough time to consider their options and make an informed choice, and do not feel forced to opt out by August 2021. Opt outs will continue to rise if people are not given the time to make an informed choice.
Theme: The GPDPR data should be managed safely and transparently inside a Trusted Research Environment.
With a Trusted Research Environments (TRE) people are not taking data out of the NHS, instead they are taking analysis results out. "This is a positive way forward and allows NHS Digital to exercise the controls we demand of it"
There should be no conflict between good research, ethics and medical care
Is IGARD (the Independent Group Advising on the Release of Data) reviewing applications for GP data?
The link to watch our previous use MY data webinar about Trusted Research Environments is available here
use MY data believes that Trusted Research Environments should become the default mechanism to ensure patient data is managed and used safely, in a way which is auditable and transparent. We are optimistic about their role in driving forward health research more rapidly and widely than other data access methods. Our principles of transparency should be adopted.
Theme: The proposed public campaign is welcomed, but more detail is needed about design, content, mechanisms and timing. The messaging about the GPDPR needs to be managed, not just left to the media.
"Can the communication strategy be a partnership approach. NHS Digital to determine the media/investment (the 'hard' bits) and others (patients; patient groups etc.) to design the messaging (the 'soft' bits)"
"I welcome the public campaign and hope that this will inform patients adequately"
We must actively inform patients and the public, rather than expecting them to find out 'by accident'
Not all people will be interested in the complexity, so some simple, clear, honest messaging is needed, with patients included in the development
This must be communicated directly to patients and the public
The detailed information, for those interested in the detail, is largely there but needs to be clarified in some areas; involvement of patients in this is essential
"To paraphrase an old advert - we are not part of a problem we are part of the solution"
use MY data believes that a robust communications plan should be developed and delivered, involving patients throughout this process. The benefits of uses of patient data for research and planning need to be emphasised.
Theme: Governance, safeguards and reporting should be clearly defined.
Patients and the public must be actively involved in decisions about appropriate uses of GPDPR data
"How can we make the public NHS data procurement contracts more transparent? There is huge concern about Palantir controlling and managing the new national GP data centre. Apparently the government is not obliged to print or make public a Data Impact Assessment (DIA) or consult on it. This must be changed for accountability and scrutiny purposes. Employers have to consult on DIAs with workers in the workplace so why doesn’t the government with the publics personal data"
"Annex B to the Direction, says that techniques will be used to reversibly anonymise the source data fields and that re-identification can be performed but only under strict governance procedures. So will NHS publish a list of entities for which data has been identified and an impact assessment for every such use"
use MY data believes that only approved users should be able to access the data. The access approval process, and the role of patients in this process, should be clear and published, as should the results of any application, whether successful or not. The GPDPR data should only be used for approved purposes to benefit the public. It should never be used for marketing or insurance purposes. If a commercial company uses patient data, the NHS must benefit fairly from any revenues generated.
Theme: Delegates' suggestions to NHS Digital, to help make the GPDPR a success.
"Contact every individual. Tell them what is happening. Be HONEST. Tell them they have a right to OBJECT and tell how and by when"
"My advice would not just be to NHS Digital (NHSD) - it would be to everyone who can help to give a more balanced platform to discuss the benefits of the actual programme and less of a platform to the privacy lobby, focused on driving opt outs by using emotive and biased language and scare tactics that does not result in 'informed' decisions. There is a reason that national organisations are afraid of transparency - because they are not given a fair trial or a fair hearing. It is all sensation, speculation and fear, fuelled by the privacy lobby and irresponsible media coverage. We all need to hold the commentarial to account as much as NHSD"
"Work with people to plan your public conversations"
"1) must get the data protection side right: need to mandate use of TRE only (NHSD's own, or an approved third party's) 2) must commit to having patient/public input to all decisions about who gets access to our valuable data 3) must tell everybody in England about the plan and give them an opportunity to choose what to do in good time ahead of implementation"
use MY data believes in listening to patients, which means seeking a range of views. We surveyed delegates after the workshop and asked if they had any specific advice for NHS DIgital. We think all these should feed into the design of the next steps.
Summary and close
Chris brought the webinar to a close, highlighting some key points made by delegates, notably one delegate asking "How is Joe Bloggs expected to find out about, and hence make an informed decision about, GPDPR?".
Chris reflected that what was pleasing to hear is that the members of the panel, with their different backgrounds, skills and experiences, actually largely agreed on most things – now we just need to put things into practice, listen to and act upon delegates' voices and those of others, and take the next steps to make this programme (to quote Phil), "safe, consensual and transparent".
Chris brought the webinar to a close saying that he was hopeful, after listening to the panellists and delegates, that there would be a way through, but it would require a collective effort.
use MY data hopes that patients will be comfortable sharing their data for planning and research, but this has to be an individual, informed choice
use MY data would like to thank all the delegates and speakers for their time and contributions. Thank you to Beth Kitchen for the title graphic and to HNE Media for their video editing support.
Contact us
email: contact@usemydata.org.uk
"the only independent patient movement in the UK focused on patient data"
use MY data is registered as a not for profit company limited by guarantee in England and Wales (14425977)